Establishing whether the diagnosis is epilepsy or not
Determining whether a patient has epilepsy requires careful evaluation. Since several conditions such as migraine, sleep disorders, panic attacks, or transient ischaemic attacks can mimic epileptic seizures, clinicians must distinguish these from true epilepsy. Diagnosis is usually based on recurrent unprovoked seizures, the probability of recurrence, or the presence of a well-defined epilepsy syndrome.
Conditions that mimic epileptic seizures
- benign paroxysmal positional vertigo
- migraine
- sleep disorders
- panic attacks
- transient ischaemic attacks
Diagnostic Evaluation
- two or more unprovoked or reflex seizures >24 hours apart
- one seizure with a ≥60% chance of recurrence in 10 years
- well-defined epilepsy syndrome with one or more seizures
After any paroxysmal events suggestive of an epileptic seizure, patients should have a full assessment, including medical history, physical exam, EEG, and neuroimaging.

Medical History:
Check for unrecognized previous seizures, as the first noticeable event may suggest epilepsy. Videos of the event can help distinguish epileptic seizures from non-epileptic events, especially in areas with limited EEG access.
Physical and Neurological Examination:
Conduct a thorough exam, noting specific signs like lateral tongue biting, which can help differentiate epileptic seizures from non-epileptic events.
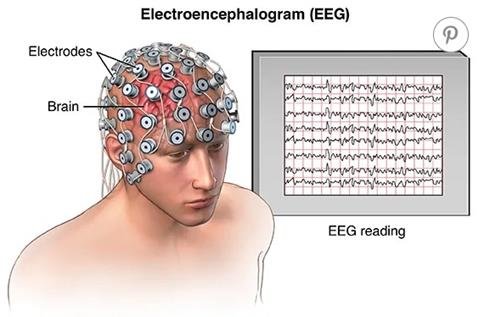
EEG:
A routine EEG helps diagnose suspected epilepsy, can help differentiate epileptic seizures from non-epileptic events, classifying types, and predicting recurrence risk. Long-term EEG or video-EEG may be needed if uncertainty persists.

Neuroimaging:
MRI is crucial for detecting epileptogenic lesions in new-onset seizures, while CT may be used initially but misses many epileptogenic abnormalities.

Genetic Testing:
Consider genetic testing, especially in severe cases like developmental and epileptic encephalopathies, as it can aid in diagnosis and guide patient management.
References
- Okudan ZV, Özkara Ç. Reflex epilepsy: triggers and management strategies. Neuropsychiatr Dis Treat. 2018 Jan 18;14:327-337. doi: 10.2147/NDT.S107669. PMID: 29403278; PMCID: PMC5779309